

By Medicine for World | mfw.com.bd
When an oncologist recommends a PARP inhibitor, patients often hear three names — Olaparib, Niraparib, and Rucaparib and have no clear way to understand what separates them. They belong to the same drug class, but they are not interchangeable. Each has different approvals, different patient selection criteria, and different side effect profiles. This guide cuts through the confusion.
the detailed article is here: https://mfw.com.bd/olaparib-vs-niraparib-vs-rucaparib/
What Is a PARP Inhibitor?
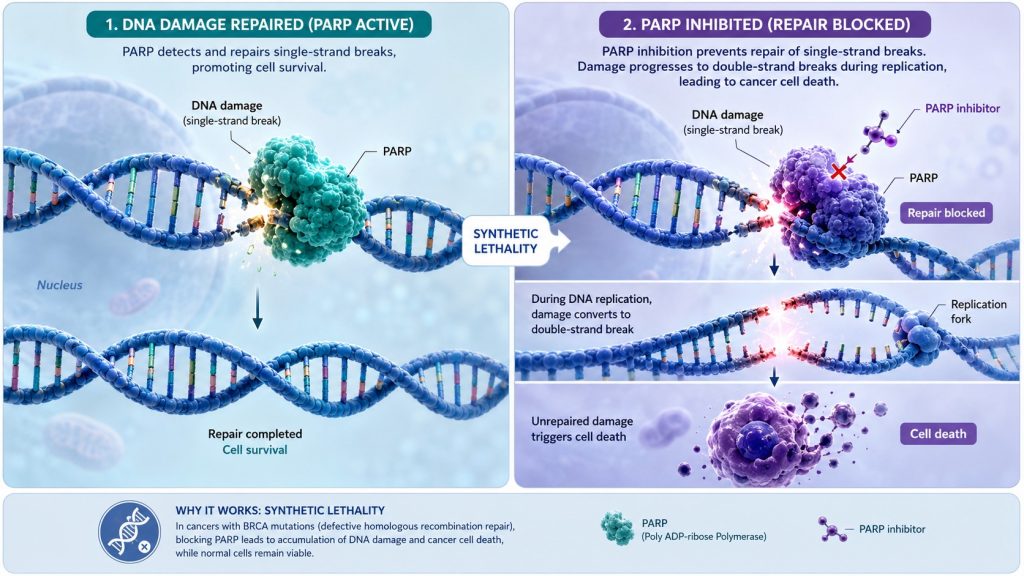
PARP stands for Poly (ADP-ribose) Polymerase — an enzyme that helps repair damaged DNA inside cells. Cancer cells rely on this enzyme to survive. PARP inhibitors block it, causing DNA damage to accumulate until the cancer cell can no longer function and dies.
This works most powerfully in patients with BRCA1 or BRCA2 gene mutations. These mutations already disable one DNA repair pathway. When PARP is also blocked, the cancer cell has no way left to fix its DNA — a concept called synthetic lethality. Healthy cells survive because they have multiple backup repair systems.
Some patients without BRCA mutations also benefit if their tumors show homologous recombination deficiency (HRD) — a broader category of DNA repair weakness that PARP inhibitors can exploit.
Olaparib (Lynparza) — The Broadest Option
Olaparib was the first PARP inhibitor approved by the FDA, in 2014. It has the widest range of approved cancer types among all three drugs.
Approved for: Ovarian, breast, prostate, and pancreatic cancers — all in patients with BRCA or relevant gene mutations.
Dosing: 300 mg twice daily.
Best for: Patients with a confirmed BRCA mutation across multiple cancer types. The SOLO-1 trial showed a median progression-free survival of 56 months in BRCA-mutated ovarian cancer patients on olaparib maintenance — compared to 13.8 months with placebo.
Common side effects: Nausea, fatigue, anemia, and decreased appetite. Generally well-tolerated with dose adjustments when needed.
Niraparib (Zejula) — The All-Comer Option
Niraparib was approved in 2017 and stands out for one important reason: it is the only PARP inhibitor approved for first-line ovarian cancer maintenance regardless of BRCA or HRD status. Oncologists do not need to wait for biomarker test results to start treatment.
Approved for: First-line and recurrent ovarian cancer maintenance therapy.
Dosing: 200–300 mg once daily (individualized by body weight and platelet count).
Best for: Newly diagnosed advanced ovarian cancer patients after a response to platinum chemotherapy, particularly when biomarker testing is unavailable or results are negative. Benefit is greatest in HRD-positive patients but extends to the broader population.
Common side effects: Low platelet count (thrombocytopenia), hypertension, nausea, and fatigue. The individualized dosing approach introduced in recent years has significantly reduced severe blood-related side effects.
Rucaparib (Rubraca) — The Narrowing Role
Rucaparib received FDA approval in 2016 but has seen its role significantly reduced. In 2022, Clovis Oncology voluntarily withdrew its prostate cancer indication after trial data showed no overall survival benefit in a broader patient population. Its commercial availability has since become limited.
Approved for: Recurrent BRCA-mutated ovarian cancer after two or more prior chemotherapy regimens.
Dosing: 600 mg twice daily.
Best for: A narrowing group — primarily BRCA-mutated recurrent ovarian cancer patients in later lines of treatment where olaparib or niraparib may not be available or suitable.
Common side effects: Nausea, fatigue, anemia, and notably elevated liver enzymes more frequently than the other two agents.
Side Effects All Three Share
Every PARP inhibitor carries a class-wide risk of myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML) — a rare but serious bone marrow condition seen in approximately 1–2% of patients. Regular blood count monitoring is essential throughout treatment. Pneumonitis (lung inflammation) has also been reported with all three drugs.
How to Choose — A Simple Framework
| Situation | Preferred Option |
|---|---|
| BRCA-mutated ovarian cancer, first-line maintenance | Olaparib or Niraparib |
| All-comer ovarian cancer, first-line maintenance | Niraparib |
| BRCA-mutated breast cancer | Olaparib |
| BRCA-mutated prostate cancer | Olaparib |
| BRCA-mutated pancreatic cancer | Olaparib |
| Recurrent ovarian cancer, later lines | Olaparib or Niraparib |
The oncologist’s final decision also factors in the patient’s kidney and liver function, existing cardiovascular conditions, other medications, and local drug availability.
Bottom Line
Olaparib leads on breadth — covering the most cancer types. Niraparib leads on accessibility — no biomarker test required for ovarian cancer maintenance. Rucaparib’s role has significantly narrowed and should be confirmed with current guidelines before consideration.
No PARP inhibitor is universally superior. The best choice is always the one matched to the right patient, in the right cancer, at the right time — guided by an experienced oncologist.
For more oncology drug guides and patient-friendly medical information, visit Medicine for World.